
Professional China Endoscopic Hemostasis - Gastroenterology Accessories Endoscopic Sclerotherapy Injection Needle – ZhuoRuiHua
Professional China Endoscopic Hemostasis - Gastroenterology Accessories Endoscopic Sclerotherapy Injection Needle – ZhuoRuiHua
Professional China Endoscopic Hemostasis - Gastroenterology Accessories Endoscopic Sclerotherapy Injection Needle – ZhuoRuiHua Detail:
Application
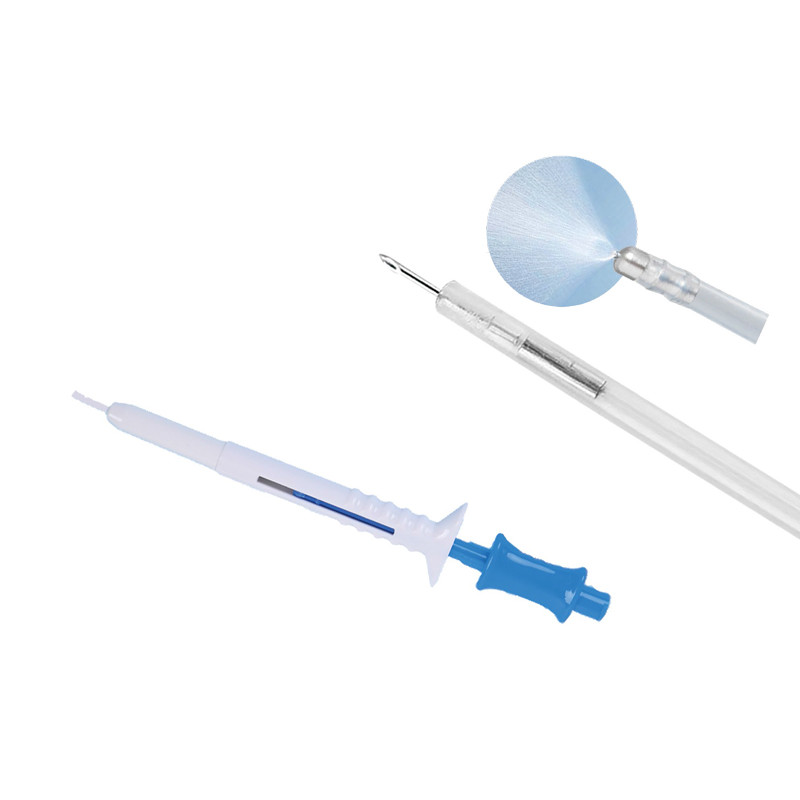
ZRHmed® Sclerotherapy needle is intended to be used for the endoscopic injection of sclerotherapy agents and dyes into esophageal or colonic varices. It is also indicated to inject saline to aid in endoscopic mucosal resection (EMR) and polypectomy procedures. The injection of saline to aid in Endoscopic Mucosal Resection (EMR), Polypectomy procedures and to control non-variceal haemorrhage.
Specification
| Model | Sheath O.D.D±0.1(mm) | Working Length L±50(mm) | Needle Size (Diameter/Length) | Endoscopic Channel (mm) |
| ZRH-PN-2418-214 | Φ2.4 | 1800 | 21G,4mm | ≥2.8 |
| ZRH-PN-2418-234 | Φ2.4 | 1800 | 23G,4mm | ≥2.8 |
| ZRH-PN-2418-254 | Φ2.4 | 1800 | 25G,4mm | ≥2.8 |
| ZRH-PN-2418-216 | Φ2.4 | 1800 | 21G,6mm | ≥2.8 |
| ZRH-PN-2418-236 | Φ2.4 | 1800 | 23G,6mm | ≥2.8 |
| ZRH-PN-2418-256 | Φ2.4 | 1800 | 25G,6mm | ≥2.8 |
| ZRH-PN-2423-214 | Φ2.4 | 2300 | 21G,4mm | ≥2.8 |
| ZRH-PN-2423-234 | Φ2.4 | 2300 | 23G,4mm | ≥2.8 |
| ZRH-PN-2423-254 | Φ2.4 | 2300 | 25G,4mm | ≥2.8 |
| ZRH-PN-2423-216 | Φ2.4 | 2300 | 21G,6mm | ≥2.8 |
| ZRH-PN-2423-236 | Φ2.4 | 2300 | 23G,6mm | ≥2.8 |
| ZRH-PN-2423-256 | Φ2.4 | 2300 | 25G,6mm | ≥2.8 |
Products Description




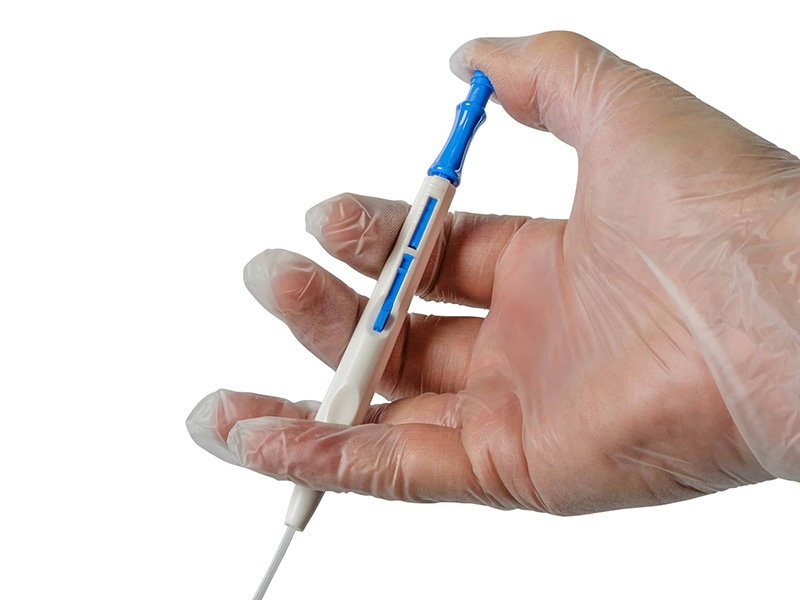
Ergonomic Handle Design
Easy to control the needle moving.
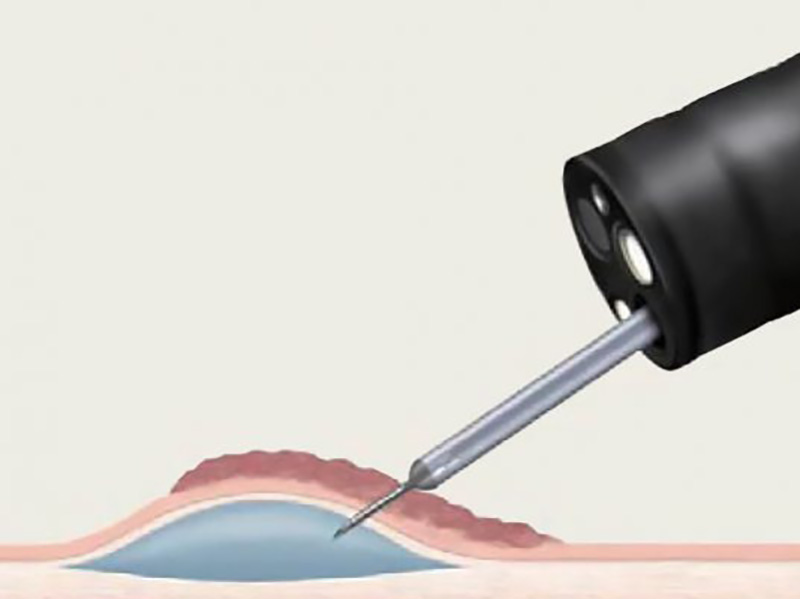
How the Disposable Sclerotherapy Needle Works
A sclerotherapy needle is used to inject fluid into the submucosal space to elevate the lesion away from the underlying muscularis propria and create a less flat target for resection.
Lift-and-cut technique for endoscopic mucosal resection.
(a) Submucosal injection, (b) passage of grasping forceps through the open polypectomy snare, (c) tightening of the snare at the base of the lesion, and (d) completion of the snare excision.
A sclerotherapy needle is used to inject fluid into the submucosal space to elevate the lesion away from the underlying muscularis propria and create a less flat target for resection. The injection is often done with saline, but other solutions have been used to achieve longer maintenance of the bleb including hypertonic saline (3.75% NaCl), 20% dextrose, or sodium hyaluronate [2]. Indigo carmine (0.004%) or methylene blue is often added to the injectate to stain the submucosa and provides a better evaluation of the depth of resection. The submucosal injection can also be used to determine if a lesion is appropriate for endoscopic resection. Lack of elevation during injection indicates adherence to the muscularis propria and is a relative contraindication to proceeding with EMR. After creating the submucosal elevation, the lesion is grasped with a rat tooth forceps that has been passed through an open polypectomy snare. The forceps lifts the lesion and the snare is pushed down around its base and resection ensues. This “reach-through” technique requires a double lumen endoscope which can be cumbersome to use in the esophagus. As a result, lift-and-cut techniques are used less commonly for esophageal lesions.
Product detail pictures:
Related Product Guide:
Our purpose is to fulfill our clients by offering golden company, great price and premium quality for Professional China Endoscopic Hemostasis - Gastroenterology Accessories Endoscopic Sclerotherapy Injection Needle – ZhuoRuiHua , The product will supply to all over the world, such as: Malta, Bangalore, Angola, Insisting over the high-quality generation line management and prospects guide provider, we have made our resolution to offer our shoppers using the initially stage purchasing and soon after provider working experience. Preserving the prevailing helpful relations with our prospects, we even now innovate our product lists the many time to meet up with the brand new wants and stick to the latest trend of this business in Ahmedabad. We're ready to facial area the difficulties and make the transform to grasp many of the possibilities in international trade.
The goods we received and the sample sales staff display to us have the same quality, it is really a creditable manufacturer.
-
Free sample for Cold Polypectomy - Single Use ...
-
New Arrival China Zebra Guide Wire With Tip - ...
-

Factory source Flexible Cystoscopy Biopsy Force...
-

China Cheap price For Ercp And Urinary - Gastr...
-

Factory source Snare Technique Colonoscopy - E...
-
Hot New Products Ercp Guidewire - Disposable S...