
Colon polyps are a common and frequently-occurring disease in gastroenterology. They refer to intraluminal protrusions that are higher than the intestinal mucosa. Generally, colonoscopy has a detection rate of at least 10% to 15%. The incidence rate often increases with age. rise. Since more than 90% of colorectal cancers are caused by malignant transformation of polyps, the general treatment is to perform endoscopic resection as soon as polyps are seen.
In daily colonoscopy, 80% to 90% of polyps are less than 1 cm. For adenomatous polyps or polyps with a length ≥ 5 mm (whether adenomatous or not), elective endoscopic resection is recommended. The possibility of colon micropolyps (length diameter ≤5mm) containing tumor components is extremely low (0~0.6%). For micropolyps in the rectum and sigmoid colon, if the endoscopist can accurately determine that they are non-adenomatous polyps, there is no need to Resection, but the above point of view is rarely implemented in clinical practice in China.
In addition, 5% of polyps are flat or grow sideways, with a diameter of more than 2 cm, with or without malignant components. In this case, some advanced endoscopic polyp removal techniques are required, such as EMR and ESD. Let’s take a look at the detailed steps for polyp removal.
Surgical procedure
The patient completed the preoperative anesthesia assessment, was placed in the left lateral decubitus position, and was given intravenous anesthesia with propofol. Blood pressure, heart rate, electrocardiogram, and peripheral blood oxygen saturation were monitored during the operation.
1 Cold/Hot Biopsy Forceps Division
It is suitable for the removal of tiny polyps ≤5mm, but there may be the problem of incomplete removal of polyps 4 to 5mm. On the basis of cold biopsy, thermal biopsy can use high-frequency current to cauterize residual lesions and perform hemostasis treatment on the wound. However, care should be taken to avoid damage to the serosa layer of the intestinal wall due to excessive electrocoagulation.
During the operation, the head end of the polyp should be clamped, lifted appropriately (to avoid damaging the muscle layer), and kept at an appropriate distance from the intestinal wall. When the polyp pedicle turns white, stop electrocoagulation and clamp the lesion. It should be noted that it is not easy to remove too large a polyp, otherwise it will prolong the electrification time and increase the risk of full-thickness damage (Figure 1).
2 Cold/hot polypectomy snare removal method
Suitable for raised lesions of different sizes I p type, I sp type and small (<2cm) I s type (specific classification standards can refer to endoscopic detection of early cancer of the digestive tract. There are too many types and I don’t know how to judge? This article Make it clear) Resection of lesions. For small type Ip lesions, snare resection is relatively simple. Cold or hot snares can be used for resection. During resection, a certain length of pedicle should be retained or a certain distance from the intestinal wall while ensuring complete removal of the lesion. After tightening the snare, it should be shaken Snare, observe whether there is surrounding normal intestinal mucosa and insert it together to prevent damage to the intestinal wall.
Figure 1 Schematic diagram of thermal biopsy forceps removal, A before forceps removal, B the wound after forceps removal. C-D: Precautions for thermal biopsy forceps removal. If the polyp is too large, it will increase the electrocoagulation time and cause transmural damage.
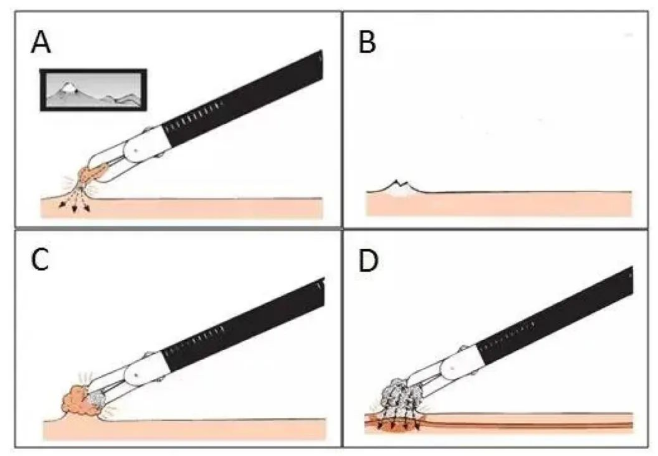
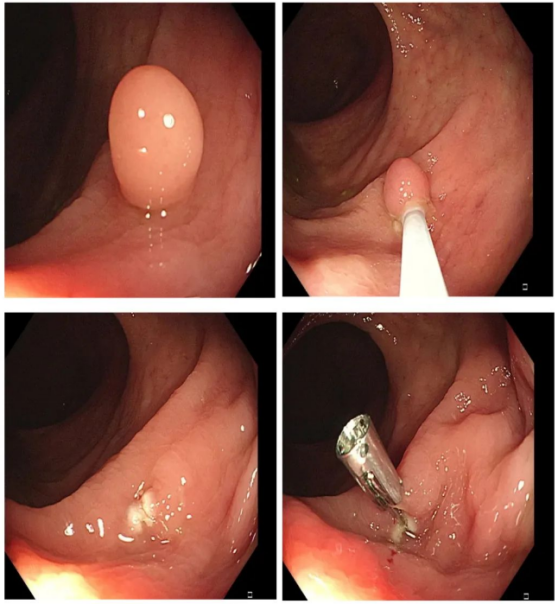
Figure 2 Schematic diagram of thermal snare resection of small I sp type lesions
3 EMR
■I p lesions
For large I p lesions, in addition to the above precautions, thermal traps should be used for resection. Before resection, sufficient submucosal injection should be made at the base of the pedicle (2 to 10 mL of 10,000 units of epinephrine + methylene blue + physiological The saline mixture is injected under the mucosa (inject while withdrawing the needle), so that the pedicle is fully raised and easy to remove (Figure 3). During the resection process, the lesion should avoid contact with the intestinal wall to avoid forming a closed loop and burning the intestinal wall.
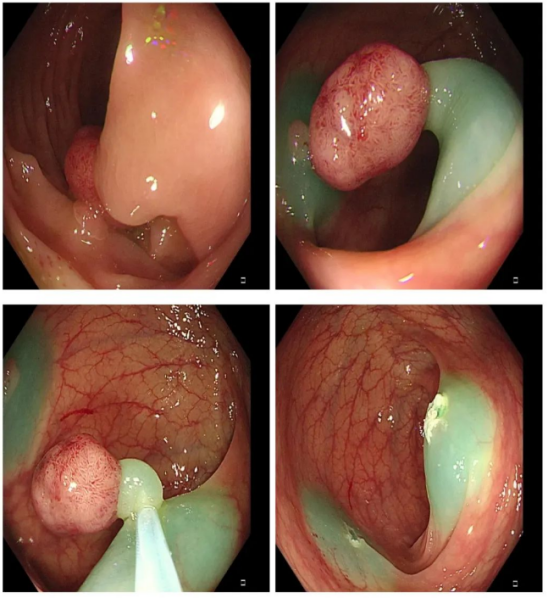
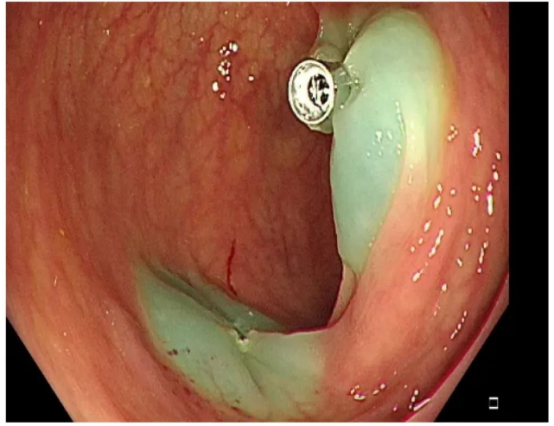
Figure 3 Schematic diagram of EMR treatment of lp-type lesions
It should be noted that if a large type I p polyp has a thick pedicle, it may contain large vasa vasorum, and it will easily bleed after removal. During the resection process, the coagulation-cut-coagulation method can be used to reduce the risk of bleeding. Some larger polyps can be resected in pieces to reduce the difficulty of the operation, but this method is not conducive to pathological assessment.
■lla-c type lesions
For Ila-c type lesions and some Is lesions with larger diameters, direct snare resection may cause full-thickness damage. Submucosal injection of liquid can increase the height of the lesion and reduce the difficulty of snare and resection. Whether there is protrusion during surgery is an important basis for determining whether the adenoma is benign or malignant and whether there are indications for endoscopic treatment. This method can increase the complete resection rate of adenomas <2cm in diameter.
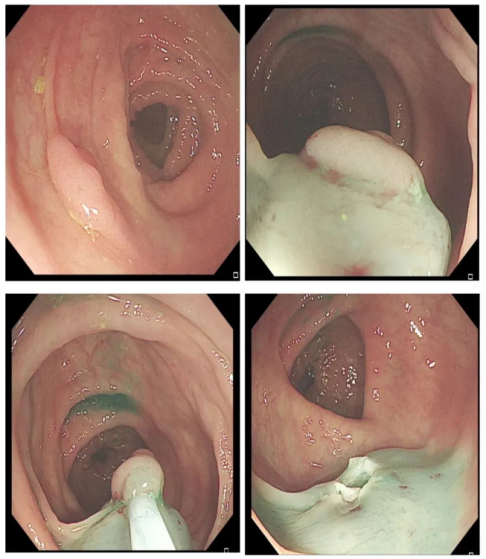

Figure 4 EMR treatment flow chart for type Il a polyps
4 ESD
For adenomas with a diameter larger than 2cm that require one-time resection and negative lift sign, as well as some early cancers, EMR residuals or recurrences that are difficult to treat, ESD treatment can be performed. The general steps are:
1. After endoscopic staining, the boundary of the lesion is clearly defined and the circumference is marked (the lesion may not be marked if the boundary of the lesion is relatively clear).
2. Inject submucosally to make the lesions obviously lifted.
3. Partially or circumferentially incise the mucosa to expose the submucosa.
4. Loosen the connective tissue along the submucosa and gradually peel off the diseased tissue.
5. Observe the wound carefully and treat the blood vessels to prevent complications.
6. After processing the resected specimens, send them for pathological examination.
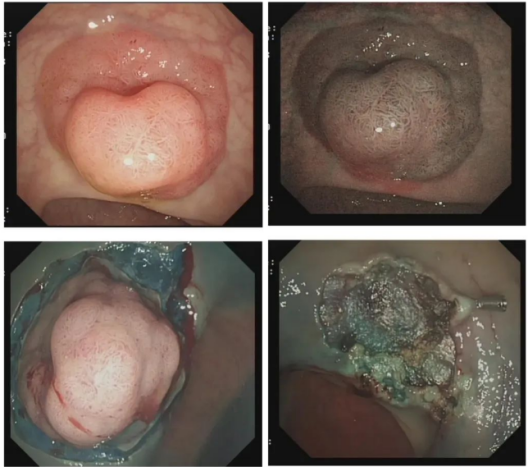
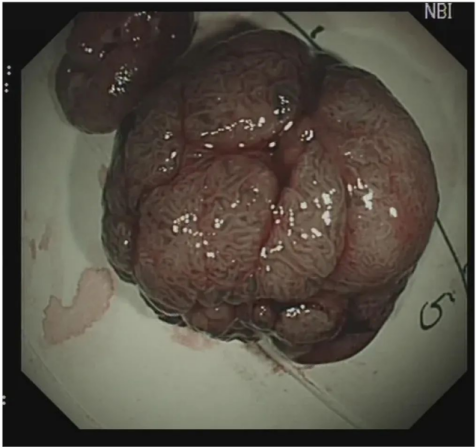
Figure 5 ESD treatment of large lesions
Intraoperative precautions
Endoscopic colon polyp resection requires an appropriate method to be selected based on polyp characteristics, location, operator's skill level, and existing equipment. At the same time, polyp removal also follows common principles, which we need to follow as much as possible to ensure that the medical process is safe and effective and patients benefit from it.
1. The pre-setting of the treatment plan is the key to the successful completion of polyp treatment (especially large polyps). For complex polyps, it is necessary to choose the corresponding resection method before treatment, communicate with nurses, anesthesiologists and other staff in a timely manner, and prepare treatment equipment. If conditions permit, it can be completed under the guidance of a senior surgeon to prevent various surgical accidents.
2. Maintaining a good "degree of freedom" on the mirror body during treatment is the prerequisite to ensure that the operation intention is realized. When entering the mirror, strictly follow the "axis maintenance and shortening method" to keep the treatment position in a loop-free state, which is conducive to precise treatment.
3. Good operating vision makes the treatment process simple and safe. The patient's intestines should be carefully prepared before treatment, the patient's position should be determined before surgery, and the polyps should be fully exposed by gravity. It is often better if the lesion is located on the opposite side of the remaining fluid in the intestinal cavity.
We, Jiangxi Zhuoruihua Medical Instrument Co.,Ltd., is a manufacturer in China specializing in the endoscopic consumables, such as biopsy forceps, hemoclip, polyp snare, sclerotherapy needle, spray catheter, cytology brushes, guidewire, stone retrieval basket, nasal biliary drainage catheter etc. which are widely used in EMR, ESD, ERCP. Our products are CE certified, and our plants are ISO certified. Our goods have been exported to Europe, North America, Middle East and part of Asia, and widely obtains the customer of the recognition and praise!

Post time: Aug-02-2024