
Introduction
The main symptoms of hemorrhoids are blood in the stool, anal pain, falling and itching, etc., which significantly affect the quality of life. In severe cases, it can cause incarcerated hemorrhoids and chronic anemia caused by blood in the stool. At present, conservative treatment is mainly based on drugs, and surgical treatment is required in severe cases.
Endoscopic treatment is a newly developed treatment method in recent years, which is more suitable for grass-roots hospitals. Today, we will summarize and sort out.
1. Clinical diagnosis, anatomy and previous treatment of hemorrhoids
Diagnosis of Hemorrhoids
Diagnosis of hemorrhoids is mainly based on history, inspection, digital rectal examination and colonoscopy. In terms of medical history, it is necessary to understand anal pain, blood in the stool, hemorrhoid discharge and reinstatement, etc. The inspection mainly understands the appearance of hemorrhoids, whether there is anal fistula of perianal inflammation, etc., and digital rectal examination needs to understand the tightness of the anus and whether there is induration. Colonoscopy needs to be aware of other diseases such as tumors, ulcerative colitis, etc. that cause bleeding. Classification and grading of hemorrhoids
There are three types of hemorrhoids: internal hemorrhoids, external hemorrhoids, and mixed hemorrhoids.
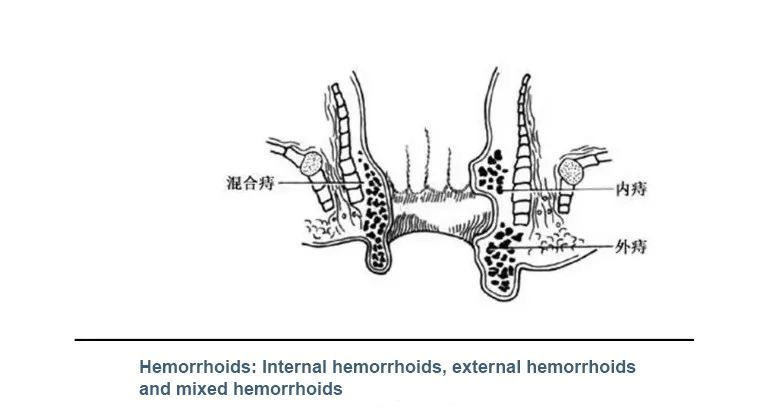
Hemorrhoids: Internal, External, and Mixed Hemorrhoids
Hemorrhoids can be classified into grades I, II, III, and IV. It is graded according to congestion, hemorrhoid discharge and return.
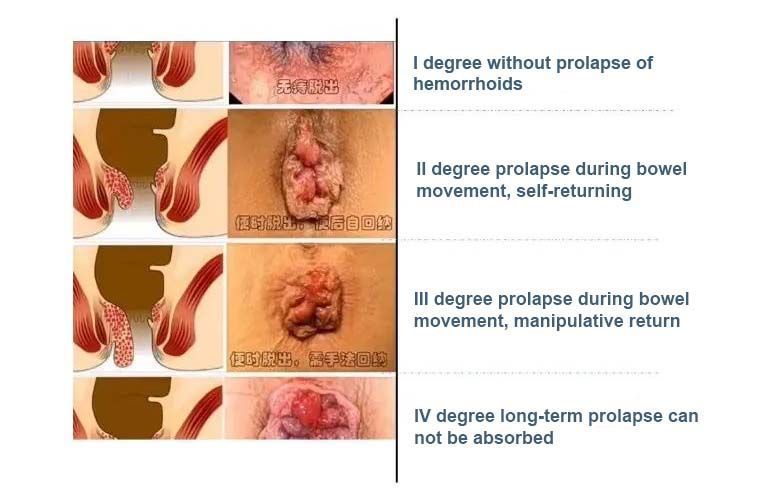
The indications for endoscopic treatment are grade I, II, and III internal hemorrhoids, while grade IV internal hemorrhoids, external hemorrhoids, and mixed hemorrhoids are contraindications for endoscopic treatment. The dividing line between endoscopic treatment is the dentate line.
Anatomy of Hemorrhoids
Anal line, dentate line, anal pad, and hemorrhoids are concepts that endoscopists need to be familiar with. Endoscopic identification requires some experience. The dentate line is the junction of the anal squamous epithelium and the columnar epithelium, and the transition zone between the anal line and the dentate line is covered by the columnar epithelium but not innervated by the body. Therefore, endoscopic treatment is based on the dentate line. Endoscopic treatment can be performed within the dentate line, and endoscopic treatment cannot be performed outside the dentate line.
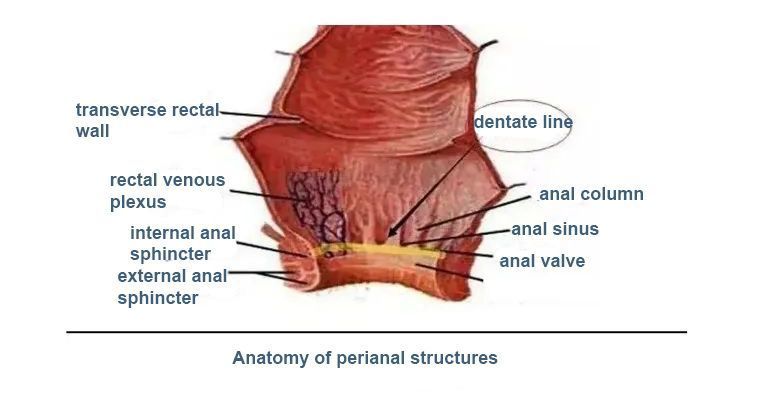
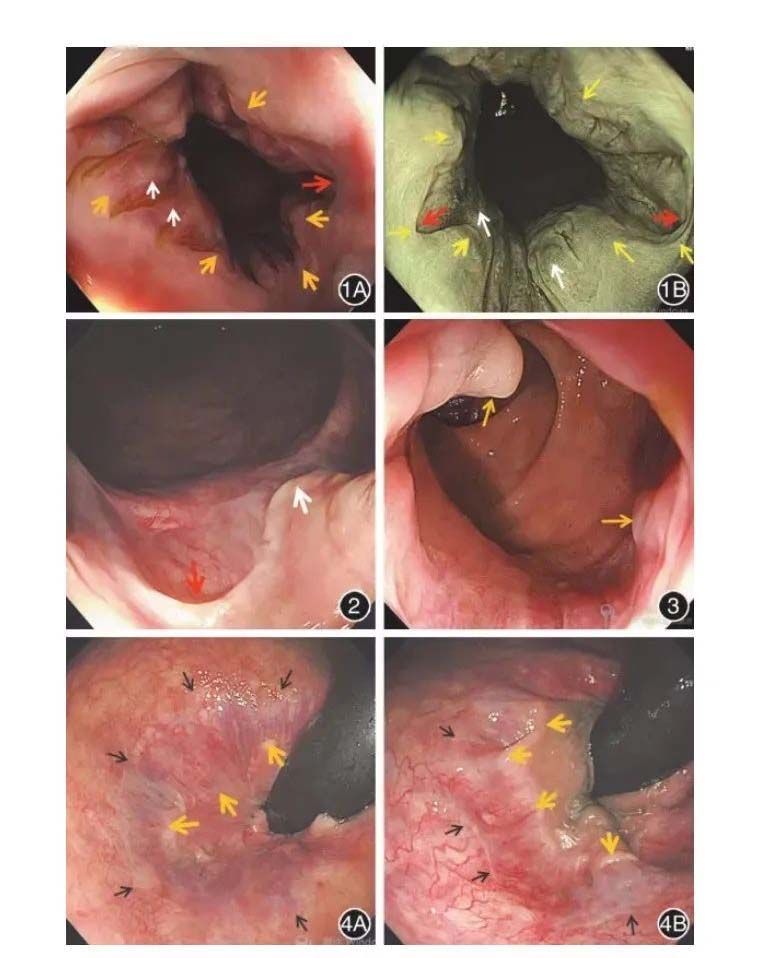
Figure 1. The frontal view of the dentate line under the endoscope. The yellow arrow points to the serrated annular dentate line, the white arrow points to the anal column and its longitudinal vascular network, and the red arrow points to the anal valve
1A: white light image; 1B: Narrowband Light Imaging
Figure 2 Observation of the anal flap (red arrow) and the lower end of the anal column (white arrow) along the microscope
Figure 3 Observation of the anal papilla along the microscope (yellow arrow)
Figure 4. The anal line and dentate line were observed by reverse endoscopy. The yellow arrow points to the dentate line, and the black arrow points to the anal line.
The concepts of anal papilla and anal column are widely used in anorectal surgery and will not be repeated here.
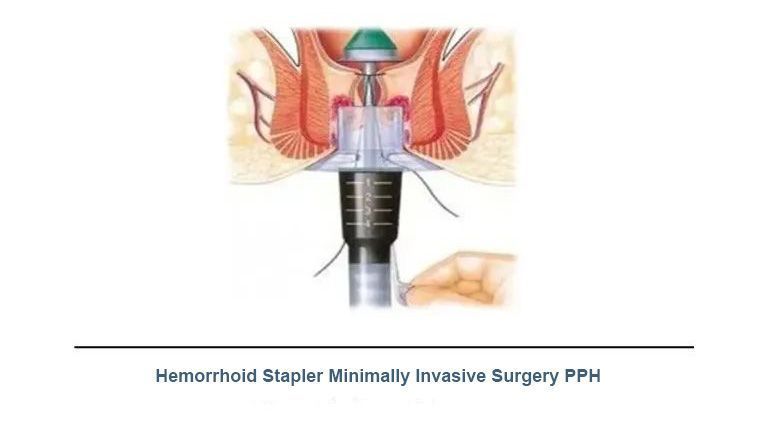
The classic treatment of hemorrhoids: there are mainly conservative treatment and surgical treatment. Conservative treatment includes drug perianal application and sitz bath, and surgical procedures mainly include hemorrhoidectomy and stapled excision (PPH). Because surgical treatment is more classic, the effect is relatively stable, and the risk is small, the patient needs to be hospitalized for 3-5 days.
2. Endoscopic treatment of internal hemorrhoids
The difference between endoscopic treatment of internal hemorrhoids and EGV treatment:
The target of endoscopic treatment of esophagogastric varices is varicose blood vessels, and the target of internal hemorrhoid treatment is not simple blood vessels, but hemorrhoids composed of blood vessels and connective tissue. The treatment of hemorrhoids is to relieve the symptoms, lift the anal pad that moves down, and avoid complications such as anal stenosis caused by the disappearance of hemorrhoids (the principle of “killing everything out” is prone to anal stenosis).
Goal of endoscopic treatment: To relieve or eliminate symptoms, not to eliminate hemorrhoids.
Endoscopic treatment includes sclerotherapy and band ligation.
For the diagnosis and treatment of internal hemorrhoids, colonoscopy is used for examination, and gastroscope is recommended for treatment. In addition, according to the actual situation of each hospital, you can choose outpatient or inpatient treatment.
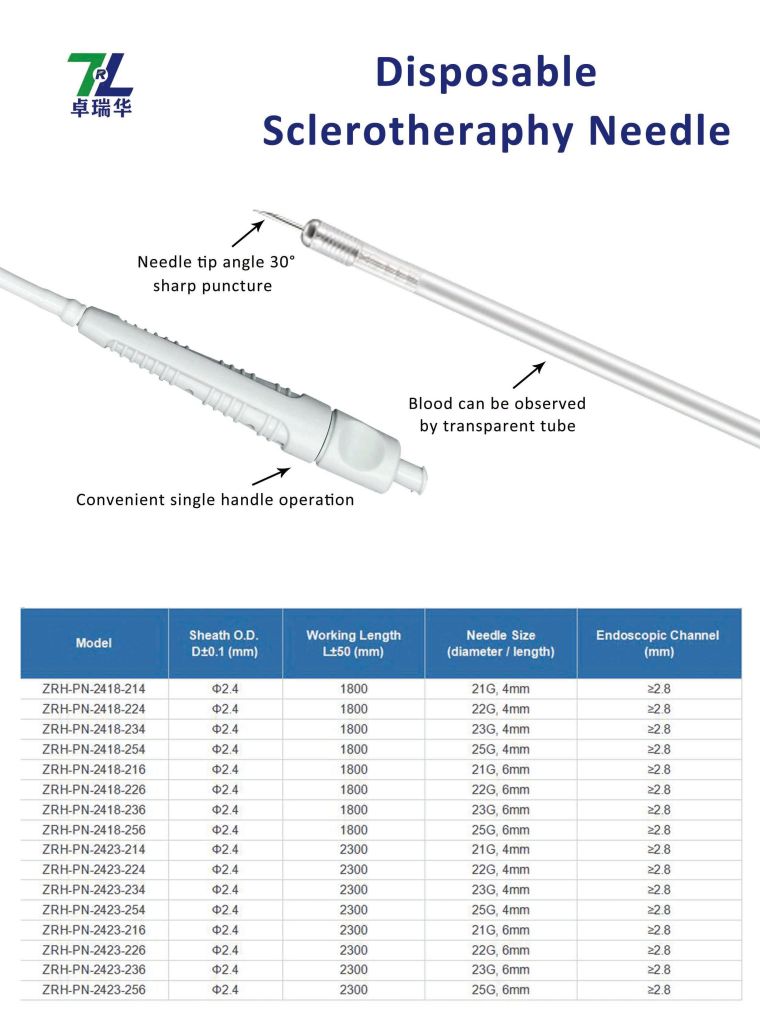
①Sclerotherapy (assisted by transparent cap)
The sclerosing agent is lauryl alcohol injection, and foam lauryl alcohol injection can also be used. It is also necessary to use submucosal injection of methylene blue as a missing agent to understand the flow direction and coverage of the sclerosing agent.
The purpose of the transparent cap is to expand the field of vision. The injection needle can be selected from ordinary mucosal injection needles. Generally, the length of the needle is 6mm. Doctors who are not very experienced should try to avoid using long needle injections, because long needle injections are prone to ectopic injection and injection. Deep risk and lead to perianal abscesses and inflammation.
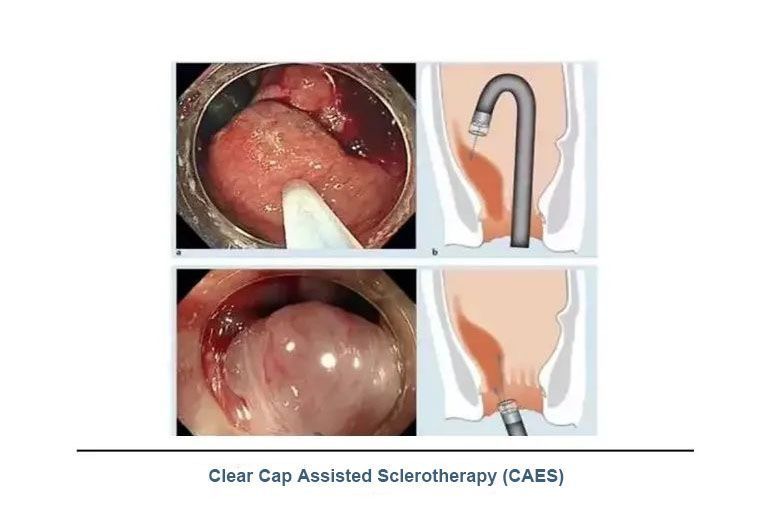
The injection point is selected above the oral side of the dentate line, and the injection needle position is located at the base of the target hemorrhoid. The needle is inserted at 30°~40° under direct vision (front or reverse) of the endoscope, and the needle is deeply inserted into the base of the hemorrhoid. Form a hardened pile at the base of the hemorrhoid, withdraw the needle while injecting, about 0.5~2mL, and stop the injection until the hemorrhoid becomes large and white. After the injection is over, observe whether there is bleeding at the injection site.
Endoscopic sclerotherapy includes front mirror injection and inverted mirror injection. Generally, inverted mirror injection is the main method.
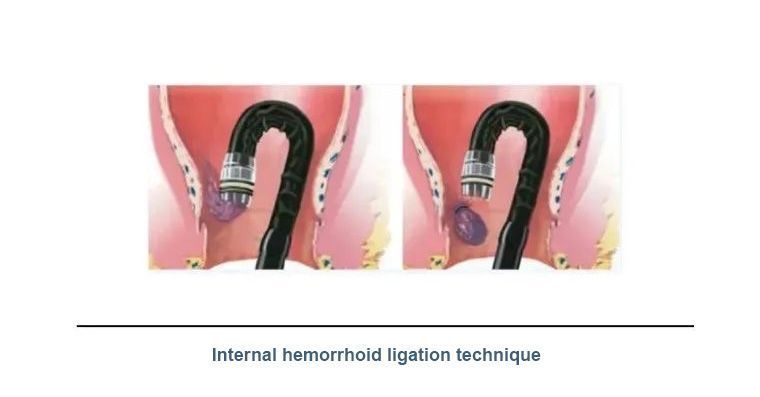
② bandage treatment
Generally, a multi-ring ligation device is used, no more than seven rings at most. The ligation is performed at 1 to 3 cm above the dentate line, and the ligation is usually started near the anal line. It can be vascular ligation or mucosal ligation or combined ligation. Inverted mirror ligation is the main method, usually 1-2 times, with an interval of about 1 month.
Perioperative treatment: fasting is not required after operation, maintain smooth stool, and avoid prolonged sitting and heavy physical labor. Routine use of antibiotics is not required.
3. The current situation and existing problems of grass-roots hospitals
In the past, the main position for the treatment of hemorrhoids was in the anorectal department. Systemic treatment in the anorectal department includes conservative medication, sclerotherapy injection, and surgical treatment.
Gastrointestinal endoscopists are not very experienced in the identification of perianal anatomy under endoscopy, and the indications for endoscopic treatment are limited (only internal hemorrhoids can be treated). Surgery is also required to make a full recovery, which has become a difficult point in the development of the project.
In theory, endoscopic treatment of internal hemorrhoids is particularly suitable for primary hospitals, but in practice, it is not as much as imagined.
We, Jiangxi Zhuoruihua Medical Instrument Co.,Ltd., is a manufacturer in China specializing in the endoscopic consumables, such as biopsy forceps, hemoclip, polyp snare, sclerotherapy needle, spray catheter, cytology brushes, guidewire, stone retrieval basket, nasal biliary drainage catheter etc. which are widely used in EMR, ESD, ERCP. Our products are CE certified, and our plants are ISO certified. Our goods have been exported to Europe, North America, Middle East and part of Asia, and widely obtains the customer of the recognition and praise!
Post time: Jul-11-2022